
Introduction
Message from PI – May 5, 2020
To students who wish to study cancer:
 The students who are reading this homepage may be undergraduate students, master degree graduate students, doctoral degree graduate students or high school students. In any case, I think you have been forced to face with a great deal of difficulty due to COVID-19. First of all, I sincerely hope that your studies and research activities will resume as soon as possible.
The students who are reading this homepage may be undergraduate students, master degree graduate students, doctoral degree graduate students or high school students. In any case, I think you have been forced to face with a great deal of difficulty due to COVID-19. First of all, I sincerely hope that your studies and research activities will resume as soon as possible.
I guess you are currently spending most of your time at home. Since I am only allowed to access to lab for the minimum research activities, I often use e-mail, Facebook and remote meeting systems for contacting staffs and students. At home, I spend a lot of time for writing and reading papers and thinking something new.
Under this situation, we happened to realize that the remote conference is very convenient. Past 10 days, I enjoyed several alumni associations over Zoom with my high school or junior high school classmates. People who occupy important positions in various occupations also participate in it. We of course heavily discussed on COVID-19. One of the things I was most impressed during the conversation was that this pandemic situation made us re-question the meaning of occupation of each one. When I heard this, I thought about myself. I am a cancer researcher and a medical doctor as well. I think it is probably admitted that doctors are needed now, but I wonder if it is the case for cancer researchers.
Our research aims to improve cancer treatment after 10 or 20 years or more. We have been investigating various things and making various suggestions, however most ideas and medicines we developed disappear without any use. For infectious disease and public health researchers who are currently trying to elucidate and overcome SARS-CoV-2, our field would look so lenient.
In Japan, it was estimated by a Professor Nishiura at Hokkaido University that about 420,000 people would die of COVID-19 if no controls were undertaken. The number of people who died from cancer in 2018 in Japan was about 370,000. A huge budget is put into cancer prevention, diagnosis and treatment in Japan. This tells us the importance of coping with COVID-19 as a policy issue.
But young people may be a little dissatisfied as even though COVID-19 rarely kill them they cannot go to school, concerts or restaurants, run out of part-time jobs, and may have a big difficulty with getting job after graduation due to presumably long-lasting economic down.
In this sense, cancer is very similar to COVID-19. The retinoblastoma that I am studying now develops in infants even just after birth, and there are many cancers that develop in early age, such as childhood cancer, so-called AYA generation cancer, leukemia, gastric cancer, etc. However, most of cancers are problems of the generation after the 60s. The movement to make more researchers engage in the study of rare cancers that occur in young people is rapidly expanding. However, given the mechanism of cancer development in which the errors in genome that accrue with aging triggers its causation, it remains a fundamental problem for the elderly. However, when I talk to various people, regardless of their age, most of them say ‘I don't want to die especially of cancer’. What is the difference between cancer and other diseases?
When I was a resident in the internal medicine department, I was in charge of various patients with malignant diseases, cardiovascular diseases, metabolic diseases and immune diseases. When a patient with acute myocardial infarction suffered a critical heart failure, all available medical staffs around there run into CCU to solve the problem. After finishing treatment, everybody returns to their own job very quickly. However, when a patient with cancer reaches his or her last moment, all the trainee doctor who were in charge of the patient gather at the bedside, and continue to stay in the room until the heartbeat stops, if patients’ family allow to do so. The next day, I saw a doctor who first diagnosed the patient standing still in front of an empty hospital room. When compared to death due to acute illness, it might be a distinct characteristic of cancer death that there are many opportunities to think carefully about the meaning of it and to taste its completion. I think many trainees have such experience and take up the challenge of postgraduate research. I was one of them.
One day, a patient with acute myelogenous leukemia (AML) died and an autopsy was performed. A green color suddenly appeared in the moment when the uterus was cut. It is a phenomenon called ‘chloroma’ in which a metabolite of protoporphyrin in leukemia cells infiltrating extramedullary organs develop color. It's unscrupulous, but I was fascinated by this phenomenone for a moment. How mysterious it is! Since I routinely stained the patient's blood sample by myself, I was surprised to see extraordinal behaviors presented by leukemic cells. When I was an undergraduate student, I was doing research on a virus that causes Adult T-cell Leukemia (ATL). But perhaps seeing this chloroma greatly affected my decision of what to do in the graduate school of medicine.
Then what is ‘cancer research’? What if we stopped all cancer treatment and research altogether? I've never seen a calculation of what happens if human beings don't treat cancer at all. However, our population had increased steadily even in era when the human beings were totally incapable of fighting against cancer. So, the effect could be biologically little. Life expectancy may a little bit shrink. However, if women can give birth to a little more children than now, the super-aged society may be resolved and a healthy society may be restored.
On the other hand, it is a natural desire for you to hope to enjoy the rest of my life and elder members of my family to live as long as possible. The fight against cancer is thus absurd. However, since President Nixon signed the Cancer Countermeasures Law (Cancer War Declaration) in 1971 and Prime Minister Nakasone formulated a 10-year comprehensive strategy against cancer in 1983, humankind started attempts to thoroughly understand and conquer cancer. These policies led to generation of innumerable number of cancer researchers including me. Humankind choose the fight against cancer almost naturally, just as they quickly prepared for COVID-19.
Even if you are not a medical doctor, there is no problem in conducting cancer research. In my lab, staffs and students from various fields such as medicine, pharmacy, biology, agriculture, nutrition, etc. gather and conduct research from various perspectives. What is cancer research for you? The answer to that question should be completely different for each individual. I don't think many people have found a clear answer. I don't think I have come to an answer yet. However, I feel that the answer will not be reached if I do not continue my research.
When I was an undergraduate student, I read the book "Virus and Cancer" (Iwanami Shinsho) and was so much impressed. I visited the author. When I asked how I should study cancer, the author immediately replied, "You do research!" The day immediately after that, my research life began and continued up to now.
Would you like to study cancer?
Our current approaches:
Ten years have passed since I established a new laboratory at the Cancer Research Institute, Kanazawa University. At the start, my lab focused on three genes Ras, RECK, and RB1. As of 2020, we are strongly focusing on RB1. RB1 is a tumor suppressor gene that has been cloned for more than 30 years. Almost all oncogenic signals promote cell cycle progression by braking on the function of the protein encoded by the RB1 tumor suppressor gene (Figure 1). In addition, the loss of RB1 function as well causes malignancy (Figure 2). We have been investigating methods to counter the malignant progression of cancer by deeply understanding the molecular mechanism of various phenomena that occur when the function of RB1 is suppressed (gain of undifferentiated phenotypes, acquisition of therapy resistance, alteration in tumor microenvironment, etc.). As a result, we came to the idea that it would be better to consider treatment methods for cancers that RB1 can still be used and cancers that RB1 can no longer be used.
Strategy to cure RB1 positive cancers
Almost all oncogenic signals enhance the function of cyclin-dependent kinases (CDKs) by enhancing D-type cyclin transactivation, and induce RB1 mono-phosphorylation, which triggers full phosphorylation of RB1 at 14 sites leading to its functional loss. Commonly used molecular targeted drugs such as Iressa, Gleevec or Trametinib block oncogenic signals upstream of D-type cyclin regulation. We are currently focusing on drugs that simultaneously inhibit the activity of CDK4 and CDK6. It restores the tumor suppressor function of RB1 by inhibiting RB1 mono-phosphorylation. In other words, it is a method of treating cancer by breaking the end point of the oncogenic signals (Figure 1). Insurance is approved for these drugs in the treatment for advanced hormone-dependent breast cancers. Chemotherapists or surgeons typically use these in combination with drugs that weaken the action of hormones. This treatment has been shown to double the disease-free survival (DFS). We are trying to elucidate the detailed molecular mechanism of the effect of this drug and the intrinsic resistance mechanism in consideration of the expanded application of CDK4/6 inhibitors to various types of cancer.
Strategy to cure RB1 negative cancers
I've been studying how to cure RB1 negative tumors for over 20 years. Loss of RB1 function not only promotes cell cycle progression but also enhances Ras oncogenic signals, intracellular metabolism (glycolysis, lipid synthesis, cholesterol metabolism, etc) and reorganization of tumor microenvironment; these help the cancer cells survive under the difficult situations. We are incubating some of the RB1 target molecules found so far as new therapeutic targets. Recently, we are also focusing on molecules such as Aurora A/B, CHK1, and PLK1 whose inhibition exert synthetic lethality when combined with RB1 loss. We are also focusing on the metabolic gene SUCLA2, which is deleted by being involved in a genomic abnormality that includes the deletion of the RB1 gene (Figure 3). We are developing a drug to treat advanced prostate cancer that lacks SUCLA2.
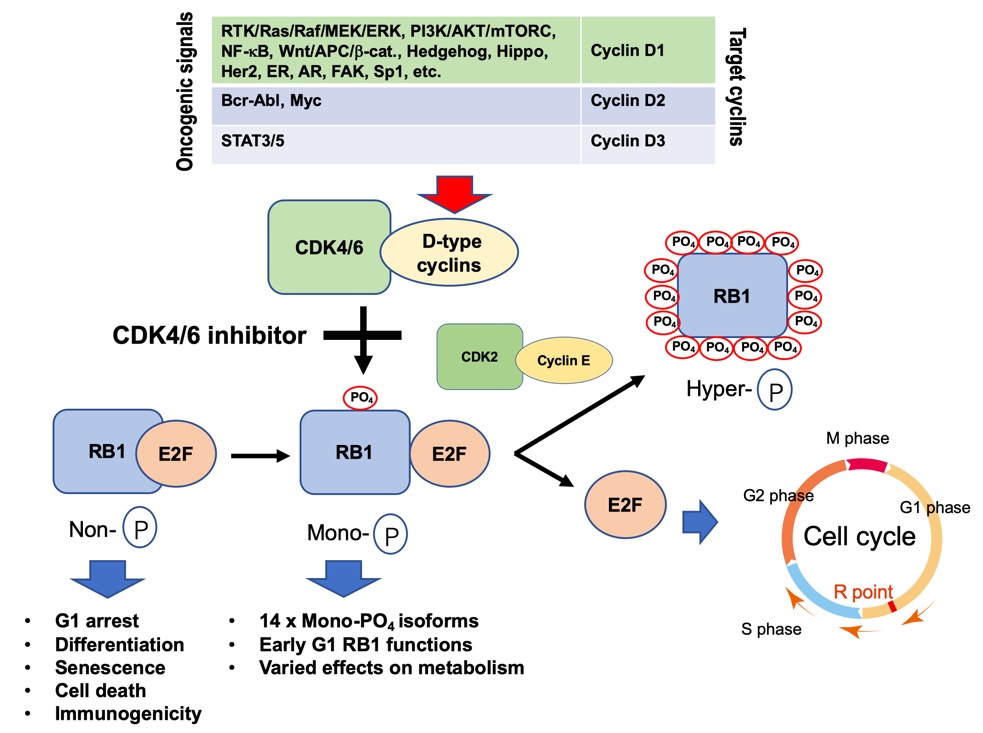
Figure 1
Almost all carcinogenic signals brake RB1 function through activation of CDK4/6.
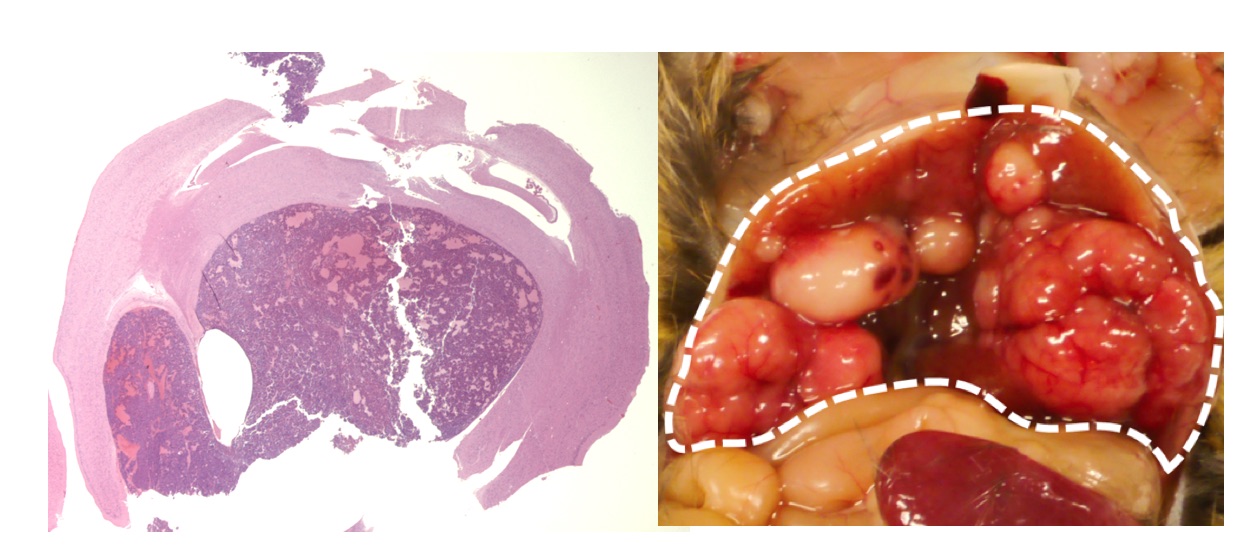
Figure 2
Brain tumor (left) and liver cancer (right) caused by suppression of RB1 function in mouse.
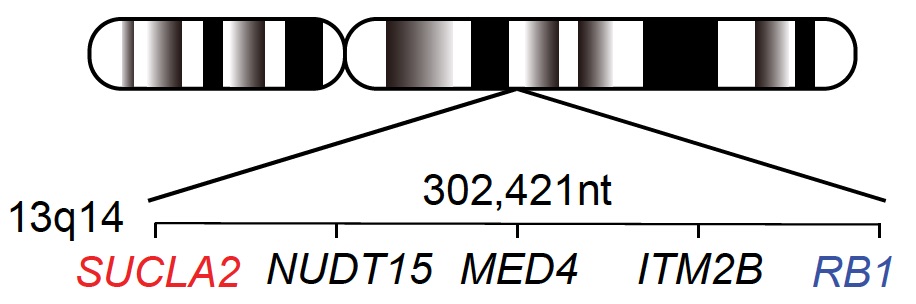
Figure 3
Simultaneous deletion of the SUCLA2 metabolic gene associated with the genomic aberration involving the RB1 tumor suppressor gene provides an Achilles’ tendon of cancer cells.
May 5, 2020
Chiaki Takahashi MD., PhD.
Message from PI 2013
 Welcome to our lab home page!
Welcome to our lab home page!
I moved my lab to Kanazawa University from Kyoto University in December 2009. Since then, we have been focusing on (i) the novel functions of the retinoblastoma tumor suppressor gene product (pRB), (ii) the mechanism of tumor-specific metabolic abnormality, and (iii) the mechanism of cancer stem cells. RB gene was isolated one-quarter century ago after in a linkage analysis of pedigrees of childhood retinal neoplasia. Even now, pRB is the most attractive molecule at least to me. Although its inactivation owing to mutation or deletion is observed in limited types of cancers, dysfunction of its product and aberration in its upstream molecules (RB pathway) are sort of hallmarks in prevailing types of cancers. We are currently particularly interested in previously unappreciated consequences of pRB inactivation during tumor progression beyond accelerated G1-S transition or differentiation defects. These include tumor angiogenesis, inflammation, metabolic reprogramming, acquisition of cancer stem-like features, etc.
I began my scientific career with Dr. Masakazu Hatanaka who is one of the leading scientists in viral oncology field; that was when I was an undergraduate at Kyoto University School of Medicine. His research group focused on proteins coded by HTLV-I viral genome that cause human adult T cell leukemia (ATL). Based on many observations, people believed that cancers were chiefly driven by disorders in genetic information. However, until 30 years ago, we did not possess firm evidence of this estimation. Infection of retroviruses carrying significantly small genomes is sufficient to transform rodent cells; this gave rise to discovery of viral oncogenes and thereafter led to identification of human oncogenes. Then, combined with discoveries of human tumor suppressor genes, the notion that cancers stem from genetic disorders was confirmed. These discoveries clearly indicated what we should target in future cancer therapy. However, I soon realized we did not yet accumulate wisdoms large enough to pursuit this. Hence, after finishing early resident course, I again moved to the basic study of human oncogenes and then tumor suppressors.
For my PhD., I joined Dr. Makoto Noda’s lab at Cancer Research Institute -JFCR and screened genes that functionally antagonize Ras-transformation in rodent cells. One of such genes, we named it RECK, appeared to inhibit number of metallo-endopeptidases and therefore control matrix invasion, angiogenesis, Notch signaling or EGFR signaling. Since the expression level of this gene significantly correlates with better prognosis of cancer patients, many physician/surgeon scientists as well as cancer biologists continue to characterize this molecule from various aspects.
For my post-doc, I joined Mark Ewen’s lab at Dana-Farber Cancer Institute. His research group noticed that pRB might exhibit some uncharacterized functions through the genetic interaction with Ras. I proved this notion by characterizing mice deficient of both Rb and N-ras. Later, my lab in Kyoto provided the mechanism of this genetic interaction as will be explained in ‘our research’. Currently, we are extending this discovery to understanding yet unveiled functions of pRB exerted during cancer progression.
As you may cleverly notice, my lab continuously work on genes of the highest clinical relevance i.e., they obtain gain-of-function or loss-of-function mutations in significant fraction of human cancers. In the era of ‘post-genome’, this direction could be no more a main stream of cancer research. However, we will continue to rely on an optimism that thorough understanding of up- or down-streams entangling with genes of strong selection pressure upon mutation must open up a roadway to conquer cancers although it may not be well paved. One testimony of such belief may be indicated in recent advances in understanding of the mechanism of metabolic reprogramming in cancer cells; number of oncogenes and tumor suppressors underlie this. We wish young students or scientists join our endeavor.
Our lab is located in Kakuma Campus of Kanazawa University. Kanazawa city accommodates approximately 450 thousands citizens which is significantly smaller than cities where I used to work, Kyoto, Tokyo or Boston. I feel time goes on much slower in Kanazawa than other cities because of atmosphere of the city and life style of people. Since very cold air from North comes across the warm current and hits against mountain area just backside of us, we have plenty of snowfall in winter season. Fortunately, Kanazawa city in winter season is also famous for gourmet food; this will probably console you many times. Of course, you can enjoy variety of winter sports without driving too far. Summer season is just wonderful in this area. I personally love summer mountaineering. Kanazawa area has Mt. Hakusan and Mt. Tateyama those are of the three greatest sacred mountains in Japan including Mt. Fuji. If you join our lab, I will introduce you to many of beautiful mountains easily accessible from Kanazawa.

Scenery from our lab of two seasons.
Our lab typically accommodates 10 people. For training students and facilitating communication with non-Japanese researchers, I strongly encourage lab people to discuss in English at lab meeting or any other occasions. Also, I love young people to autonomously drive lab and their studies. Two most important aims of our lab are (i) making very good contribution to cancer science field and (ii) generating next generation PIs. So, I always treat lab staffs and students as possible candidates of future PIs. If you are interested in my lab, please do not hesitate to contact me.
January 6, 2013
Chiaki TAKAHASHI

Lab members in 2011.